University of Kerbala
University of Kerbala

The term diastema refers to the gap or spaces between the teeth. A frequent site of a diastema is between maxillary central incisors, so make it most noticeable. The esthetic significance of a diastema and the decision to close it is predominantly the choice of the patient. Diastema can form in both children and adults, but the child has a chance that the midline spaces spontaneously decrease in size with age.
There are many possible causes for diastema, such as the presence of fibrous labial frenum that often prevents the normal approximation of erupting central incisors. The other causes are congenitally missing or supernumerary teeth, inter-arch tooth size discrepancies, and midline pathology. Diastemas may also result other problems such as oral habit (tongue thrusting or thumb sucking).
To closing diastemas, there are many treatment options: Orthodontic, direct composite, ceramic veneers or crowns. The underlying cause of an individual’s diastema and its severity will determine the treatment plan.
The direct composite restorations can be considered a more conservative, economical, and quicker option for diastema closure.
Composite veneers can be placed directly for both maxillary central incisors in a single visit. Furthermore, they can be repaired easily compared to costly and time-consuming repairs or remakes for porcelain alternatives. There the two methods for composite build up restoration: (Free hand or silicon guided techniques). Unfortunately, composite restoration has some disadvantages compared to indirect restoration. Composites can stain, chip, and lose luster and required maintenance recalls. However, the advancement in adhesive dentistry and the improvement of materials give the dentist the chance of creating esthetic, functional, economical, direct composite restoration in a short time.
Case report:
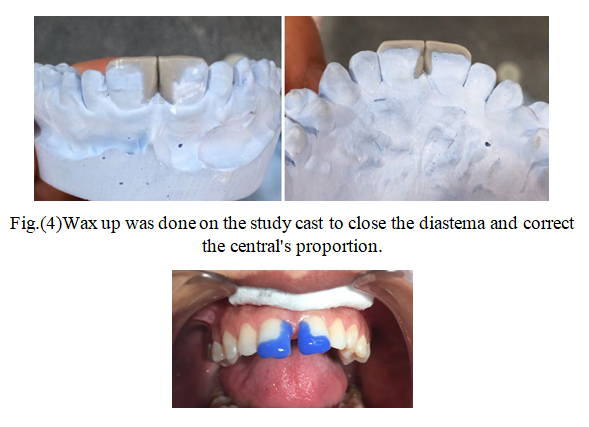
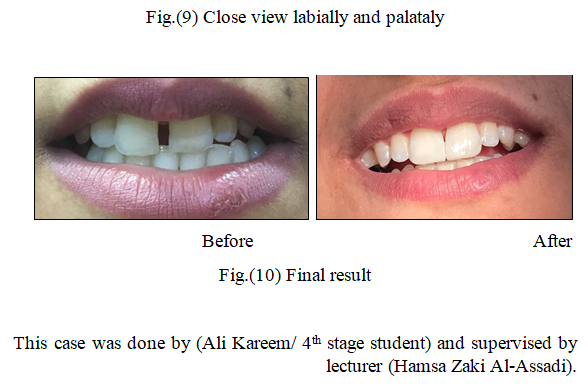
A (35 yrs. old) female patient came to the (Training Dental Clinics/ Department of Restorative Dentistry, Karbala University) with the chief complaint of midline diastema about (2mm) in the maxillary arch. We decided to close the diastema and correct the proportion of the two centrals with direct composite using silicon index as it a more esthetic, precise and economical option.